Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
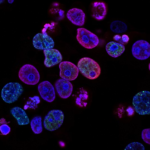
Traditional chemotherapy kills rapidly dividing cells throughout the body, which affects both malignant and healthy tissue. Antibody Drug Conjugates, or ADCs, offer a different mechanism. They combine an antibody with a cytotoxic drug. The antibody binds to specific antigens found on cancer cells. The drug payload is then released inside the target cell. This design aims to concentrate the therapeutic effect at the tumor site while reducing exposure to healthy tissues.
An ADC consists of three components. A monoclonal antibody serves as the targeting agent. A potent chemotherapy agent acts as the payload. A chemical linker connects the two and is designed to release the payload only after the ADC has entered the cancer cell. Once the ADC binds to its target antigen, the complex is internalized. Inside the cell, the linker degrades or is cleaved, allowing the cytotoxic drug to kill the cell from within. This differs from conventional chemotherapy, which distributes throughout the bloodstream and affects all rapidly dividing cells regardless of their origin.
One ADC, Enhertu, has been studied extensively in HER2 positive breast cancer. In patients with residual disease after initial treatment, Enhertu showed a lower rate of recurrence compared to older ADCs. A majority of treated patients remained free of invasive disease at follow up intervals. Another ADC, Padcev, has been evaluated for advanced bladder cancer. When used in combination with an immunotherapy agent, Padcev extended the time before cancer progression and improved overall survival relative to standard chemotherapy. Quality of life measures did not decline with the combination treatment.
The clinical use of ADCs has expanded to rare cancers. The FDA approved the first ADC for blastic plasmacytoid dendritic cell neoplasm, an aggressive blood cancer with a low incidence rate. In clinical trials, a majority of newly diagnosed patients achieved complete remission. This approval indicates that ADC technology can be applied to orphan diseases as well as common cancers.
Current ADCs have limitations. Solid tumors can develop resistance by mutating surface antigens or altering intracellular pathways. Researchers are developing next generation ADCs to address these challenges. Bispecific ADCs are designed to bind two different antigens on the same cancer cell, which reduces the likelihood of escape through antigen loss. Dual payload ADCs carry two distinct chemotherapy agents. This approach allows simultaneous attack through multiple mechanisms, potentially overcoming resistance. Several of these candidates are in human trials for lung, colorectal, and ovarian cancers.
Beyond oncology, ADC technology is being explored for infectious diseases and autoimmune conditions. The same principle of targeted delivery could apply to infected cells or pathogenic immune cells. The platform continues to evolve with refinements in linker chemistry, antibody engineering, and payload selection. These developments are expanding the range of treatable conditions and improving the therapeutic index of potent drugs that were previously too toxic for systemic use.