Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
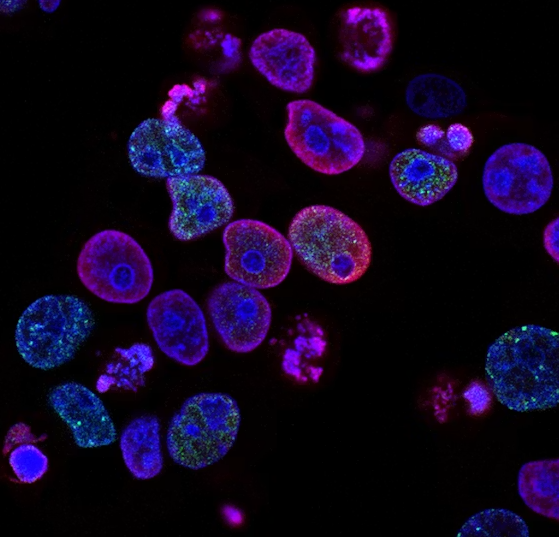
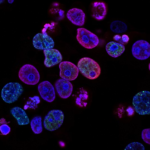
Pancreatic cancer has long been one of the most difficult cancers to treat. About ninety percent of patients with pancreatic ductal adenocarcinoma, the most common form of the disease, carry mutations in RAS genes. For decades, researchers considered these mutations impossible to target with drugs. A new oral medication called daraxonrasib may be changing that outlook.
RAS genes are among the most frequently mutated oncogenes in human cancer. They account for more than 200,000 new cancer cases per year in the United States alone. In pancreatic cancer, the most common RAS mutations occur at three specific locations on the gene. Traditional chemotherapy has limited effectiveness against these mutations. Patients with metastatic pancreatic cancer often have few good options after initial treatment fails.
Daraxonrasib, previously known as RMC 6236, takes a different approach from standard chemotherapy. It is an oral, direct RAS inhibitor that targets the active state of RAS proteins. The drug uses what researchers call a tri complex mechanism. It binds to an intracellular chaperone protein called cyclophilin A, and together they attach to the active form of RAS, blocking its ability to send growth signals to cancer cells. This approach allows daraxonrasib to inhibit a broad spectrum of KRAS mutations, including those most common in pancreatic cancer.
In a phase one and phase two trial involving 168 patients with previously treated advanced RAS mutated pancreatic cancer, researchers tested daraxonrasib at doses ranging from 10 to 400 milligrams once daily. The 300 milligram dose was selected for further study. Among 26 patients with RAS G12 mutations who received daraxonrasib as second line therapy at the 300 milligram dose, nine patients, or thirty five percent, showed an objective response. One patient achieved a complete response. The median duration of response was 8.2 months. Median progression free survival reached 8.5 months, and median overall survival was 13.1 months. Among a broader group of patients with RAS mutations treated at the same dose, the objective response rate was twenty nine percent, with median overall survival of 15.6 months.
These results compare favorably with existing second line chemotherapy options. For example, the FDA approved combination of nanoliposomal irinotecan plus fluorouracil for second line pancreatic cancer has a confirmed response rate of about seven percent.
The most common side effect reported in the trial was rash, occurring in eighty eight percent of patients. Other frequent side effects included diarrhea in forty six percent, nausea in forty two percent, and mouth sores in forty percent. Treatment related adverse events of grade three or higher, meaning more severe side effects, occurred in about thirty percent of patients. Only one patient discontinued treatment due to side effects. Most side effects were manageable with dose adjustments.
The FDA has granted Breakthrough Therapy Designation to daraxonrasib for the treatment of patients with previously treated metastatic pancreatic cancer harboring KRAS G12X mutations. This designation is intended to expedite the development and review of drugs that show substantial improvement over existing therapies. In October 2025, Revolution Medicines also received a National Priority Voucher for daraxonrasib under an FDA pilot program, which provides an expedited review process.
A global phase three trial called RASolute 302 is currently underway comparing daraxonrasib to standard of care chemotherapy in patients with previously treated metastatic pancreatic cancer. An expected data readout from that trial was anticipated in 2026. If confirmed in larger studies, daraxonrasib could become a new treatment option for patients facing this challenging disease. For now, the drug represents a measured but meaningful step forward in targeting a mutation that has resisted effective treatment for many years.